


Improving NCLEX-RN Outcomes Through an Integrated Systems Approach: The Joyce University Model and Evidence-Informed Strategies for Nursing Programs
Shelley A. Johnson, PhD, EdD, MSN, MBA, RN, NE-BC, CNETami Rogers, PhD, DVM, MSN, RN, CNE
Jun 16, 2026
Abstract
NCLEX-RN outcomes remain one of the most visible indicators of nursing program effectiveness, academic quality, regulatory confidence, and graduate readiness for entry-level nursing practice. Persistent low first-time pass rates create significant institutional risks, including heightened regulatory scrutiny, accreditation concerns, reputational harm, enrollment instability, and diminished student confidence. Historically, many nursing programs have attempted to improve outcomes through isolated interventions such as standardized testing requirements, remediation mandates, curriculum revisions, or high-stakes progression gates. These approaches may produce temporary improvement but often fail to create sustainable outcomes because NCLEX success is not the result of a single course, assessment, or remediation experience. Rather, NCLEX performance reflects the functioning of an academic ecosystem that includes curriculum design, assessment validity, faculty capability, student support, policy alignment, predictive analytics, and operational processes that support timely testing.
This paper describes the Joyce University Comprehensive NCLEX Readiness Model as an integrated, data-driven system designed to improve first-time NCLEX-RN pass rates, reduce time-to-test, strengthen readiness decisions, and support sustainable continuous improvement. The paper then translates the Joyce model into broader evidence-informed strategies that nursing programs can use to improve NCLEX-RN outcomes within accreditation and regulatory expectations. The model is aligned with the Next Generation NCLEX emphasis on clinical judgment, the AACN Essentials competency-based framework, CCNE expectations for licensure outcomes and continuous improvement, and ACEN expectations for outcomes assessment and program effectiveness.
Keywords: NCLEX-RN, Next Generation NCLEX, nursing education, predictive analytics, remediation, curriculum alignment, accreditation, clinical judgment, ATI Comprehensive Predictor, continuous quality improvement
Key Takeaways
- NCLEX-RN outcomes are vital for nursing program effectiveness, but low pass rates cause institutional risks.
- The Joyce University Comprehensive NCLEX Readiness Model offers a data-driven system for improving first-time pass rates and readiness decisions.
- This model integrates curriculum design, faculty development, assessment quality, and student support for sustainable outcomes.
- Recommendations include establishing a multi-indicator readiness model, early alert systems, and continuous program improvement processes.
- The Joyce model aligns with accreditation standards and focuses on enhancing overall educational quality, not just test preparation.
Table of contents
- Abstract
- Introduction
- The Joyce University NCLEX Readiness Model
- Assessment and Evaluation
- Faculty Development
- NCLEX Readiness Infrastructure
- Policy Alignment
- Student Support Systems
- Curriculum Design
- Evidence Supporting the JoyceU Model
- Outcome Metrics and KPI Tables
- Accreditation and Regulatory Implications
- Recommendations for Nursing Programs Seeking to Improve NCLEX-RN Outcomes
- Discussion
- Conclusion
- References
- Appendix A
Introduction
NCLEX-RN outcomes are a critical measure of nursing program effectiveness because they represent the point at which academic preparation is externally validated through a national licensure examination. For nursing programs, first-time NCLEX-RN pass rates serve multiple purposes. They are indicators of graduate readiness, markers of program quality, signals to prospective students, and evidence used by boards of nursing and accreditors to assess whether programs are meeting expected outcomes.
The launch of the Next Generation NCLEX on April 1, 2023, increased the importance of clinical judgment preparation across nursing curricula. The NGN was designed to better measure candidates’ clinical judgment and decision-making abilities through innovative item types and case-based measurement approaches (National Council of State Boards of Nursing [NCSBN], 2023a). The NCSBN Clinical Judgment Measurement Model provides a framework for measuring clinical judgment with psychometric rigor and was developed through literature review, expert input, and analysis of data from more than 200,000 NCLEX candidates (NCSBN, 2023b). This shift requires nursing programs to move beyond content coverage and toward intentional development of clinical reasoning, prioritization, cue recognition, hypothesis generation, action planning, and outcome evaluation. The JoyceU Model was reviewed with the 2026 NCLEX (NGN) update. The 2026 NCLEX -RN changes were minimal and did not force consequential changes to the JoyceU Model.
Low NCLEX-RN pass rates are rarely caused by one problem. They often reflect cumulative weaknesses in curriculum sequencing, course rigor, assessment quality, student support, faculty development, academic policies, admissions processes, and post-graduation testing support. Therefore, sustainable improvement requires a systems approach rather than a single intervention. The Joyce University Comprehensive NCLEX Readiness Model (JoyceU Model) provides one example of how a nursing program can organize NCLEX improvement as an integrated ecosystem.
The Joyce University NCLEX Readiness Model
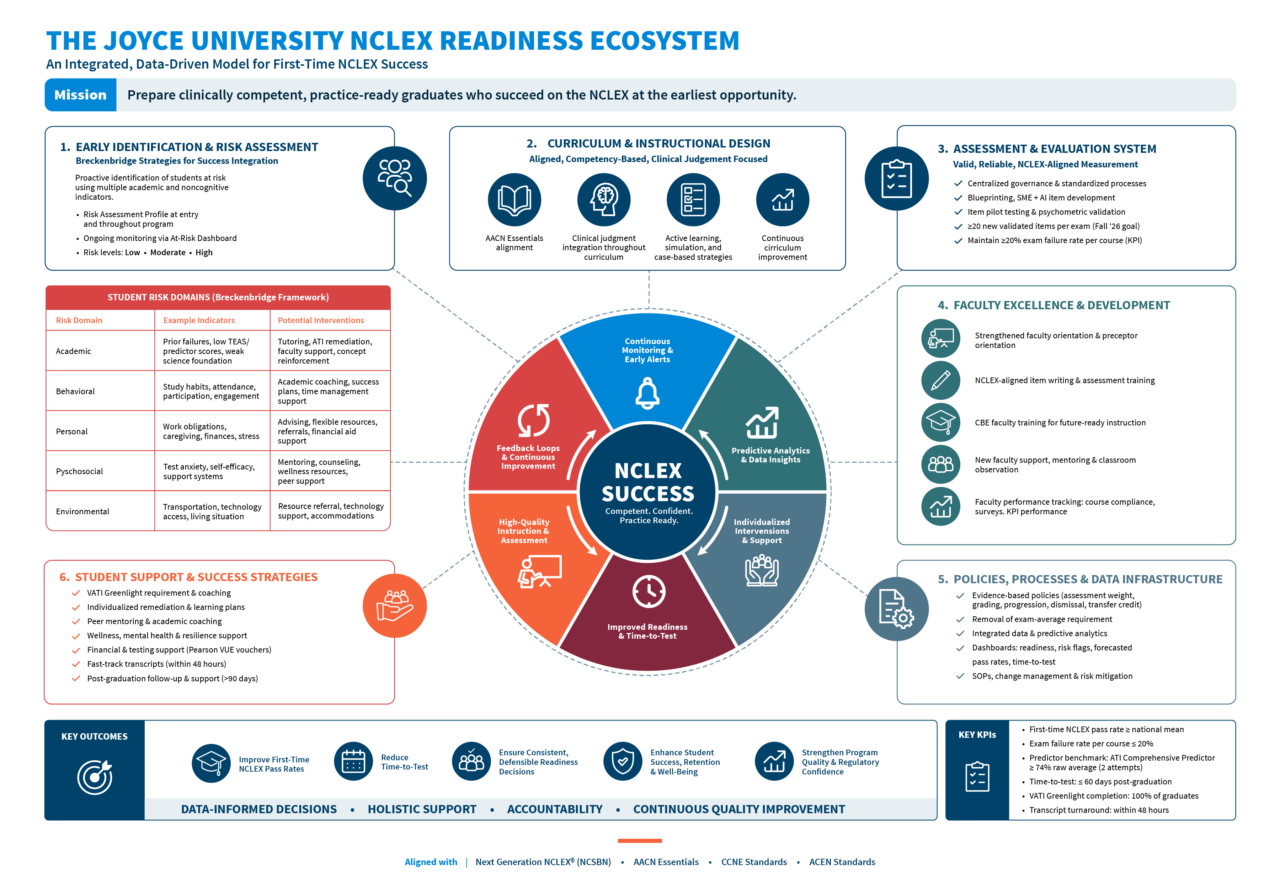
Joyce University developed a comprehensive NCLEX readiness system to improve first-time NCLEX pass rates, reduce time-to-test, and ensure consistent and defensible readiness decisions. This work integrated several components of the Diane M. Breckenridge, Zane R. Wolf, and Mary J. Roszkowski (2012) Risk Assessment Profile and Strategies for Success framework. Dr. Johnson introduced the model to Joyce University after applying and observing successful implementation at other institutions with historically lower NCLEX performance. Johnson and Rogers adapted and expanded the model for use at Joyce University. The model was further tailored to address the specific needs of Joyce students through collaboration with academic leaders, including Dean Jennifer Ayotte, Dr. Becky Collins, Dr. Ashley Otto, Assistant Dean Jennifer Cowherd, Dr. Cory Myers, and Dr. David Haskell. The model is intentionally organized as an integrated ecosystem rather than a collection of isolated initiatives. It includes six interdependent domains: assessment and evaluation, faculty development, NCLEX readiness infrastructure, policy alignment, student support, and curriculum design.
The JoyceU model is grounded in a central premise: NCLEX success is designed, measured, managed, and continuously improved. This differs from traditional approaches that place responsibility primarily on students near the end of the program. In the Joyce model, readiness begins at admission and orientation, continues through course-level assessment and remediation, is reinforced through curriculum and faculty development, and is supported through operational processes that help graduates test promptly.
Assessment and Evaluation
Joyce University implemented a comprehensive assessment and evaluation model to ensure consistent, valid, NCLEX-aligned measurement of student readiness. The model includes centralized governance, standardized blueprinting, subject matter expert review, AI-assisted item development, unbiased item review, item piloting, and psychometric validation. Exam item piloting was planned to began in Spring 2026, with the goal of developing at least 20 validated new items per exam beginning Fall 2026. The institution also established a key performance indicator to maintain exam failure rates at or below 20% per course beginning Summer 2026.
This assessment strategy recognizes that poor exam quality can distort readiness decisions. If course exams are not psychometrically sound, students may pass courses without demonstrating readiness or fail courses because of flawed items, misaligned content, or inconsistent rigor. Valid assessment systems, therefore, protect students, faculty, programs, and the public. These Joyce-content specific exams were given, along with the standardized, nationally-normed ATI subject-specific Content Master Series examinations in select courses throughout the pre-licensure programs.
Faculty Development
The Joyce model positions faculty development as a core NCLEX readiness intervention. Faculty influence curriculum delivery, classroom rigor, assessment validity, clinical judgment development, remediation quality, and the consistency of student expectations. Joyce strengthened program-specific faculty orientation, developed NCLEX-aligned item-writing and assessment training, prepared faculty for competency-based education, and created a new faculty support and readiness model that includes onboarding, observation, mentoring, and performance monitoring.
Faculty performance data are used to monitor course launch and closure compliance, end-of-course surveys, Content Mastery Series outcomes, predictor performance, and NCLEX pass rates. This approach reframes faculty development as an accountability and improvement system rather than a one-time orientation activity.
NCLEX Readiness Infrastructure
Joyce University revised its readiness infrastructure by replacing a single high-stakes predictor standard with a multi-indicator readiness model. A revised ATI Comprehensive Predictor benchmark of at least 74% raw average across two attempts replaced the prior single-attempt 95% probability-of-passing requirement. Remediation was required and guided based on each student’s individual learning needs. This change was designed to reduce high-stakes pressure while encouraging sustained preparation and allowing more students who demonstrated readiness to progress.
The ATI RN Comprehensive Predictor is designed to provide a numeric indication of a student’s likelihood of passing the NCLEX-RN and to guide remediation based on missed content (Assessment Technologies Institute [ATI], 2020). ATI’s technical documentation links percent-correct score ranges to predicted probability of passing, including a 74.0% to 74.7% range associated with an estimated 94% to 95% probability of passing the NCLEX-RN (Assessment Technologies Institute, 2020). However, Joyce’s model appropriately uses the predictor as one component of readiness rather than as a stand-alone determinant.
Joyce also incorporated VATI Greenlight requirements, weekly NCLEX data infrastructure, predictive analytics, Pearson VUE voucher incentives, and fast-track transcript processes. These strategies are designed to provide individualized readiness coaching, reduce financial and administrative barriers, and shorten the time between graduation and NCLEX testing.
Policy Alignment
The Joyce model includes systematic policy review because academic policies can either support or undermine readiness. The institution reviewed transfer credit, grading scale, dismissal and appeals, course expiration, assessment expiration, and entrance assessment policies. It also increased the weight of CMS assessments and removed reliance on an in-course exam-average requirement as the sole high-stakes determinant of progression.
The purpose of policy alignment is not to weaken standards. Rather, it is to ensure that standards are valid, equitable, evidence-informed, consistently implemented, and linked to licensure readiness. A defensible readiness system should avoid overreliance on a single high-stakes measure when multiple indicators can provide a more accurate picture of student readiness.
Student Support Systems
Joyce implemented proactive student support systems that identify risk early and intervene before failure occurs. The model includes at-risk dashboards, individualized remediation plans, key concept reviews, ATI CMS-based study plans, learning support services, re-entry safety and success plans, and redesigned new student orientation. Risk indicators include Comprehensive Predictor performance below 74%, CMS performance below benchmark, any single course examination below 80%, and course averages below 77%.
The student support model is designed to shift the institution from reactive remediation to predictive intervention. Rather than waiting until students fail a course or fail the NCLEX, the system identifies risk during the program and deploys targeted supports.
Curriculum Design
Curriculum alignment is central to the Joyce model. The institution strengthened alignment between Joyce-developed curriculum and ATI resources, improved course sequencing, mapped courses to the NCLEX blueprint, AACN Essentials, and program outcomes, and emphasized integrated learning across didactic, lab, simulation, and clinical environments.
This curricular design reflects the NGN emphasis on clinical judgment. Students must not only recall nursing content but also recognize cues, analyze data, prioritize hypotheses, generate solutions, take action, and evaluate outcomes. Therefore, NCLEX improvement requires curriculum structures that repeatedly develop and assess clinical judgment across the program.
Conceptual Figure: The Joyce University NCLEX Readiness Ecosystem

Evidence Supporting the JoyceU Model
NGN and Clinical Judgment
The NGN requires programs to prepare students for complex clinical decision-making rather than content recall alone. NCSBN describes the NGN as an exam designed to better measure clinical judgment and decision-making abilities through innovative item types (NCSBN, 2023a). The NCJMM provides a framework for valid measurement of clinical judgment and decision-making within the NCLEX context (NCSBN, 2023b). These developments support Joyce’s emphasis on curriculum alignment, clinical judgment assessment, simulation integration, and progressive complexity across the program.
Predictive Analytics and Multiple Readiness Indicators
The literature supports the use of multiple predictors rather than a single readiness measure. Cummings et al. (2024) found that GPA and the ATI Comprehensive Predictor both accurately classified 86.67% of NCLEX-RN success, while performance in anatomy and physiology and pathophysiology classified 84.81% of NCLEX-RN success. ATI Medical-Surgical scores and the ATI Comprehensive Predictor were also correlated with first-time NCLEX-RN success. These findings support a multi-indicator model that includes academic performance, course-specific standardized assessments, and comprehensive predictors.
The ATI Comprehensive Predictor technical documentation states that the assessment is intended to estimate readiness and guide remediation; it also cautions that institutions using the exam are responsible for decisions based on test scores (Assessment Technologies Institute, 2020). This distinction is important. Standardized predictors can inform readiness decisions, but program leaders should avoid treating them as the only evidence of readiness. Joyce Nursing Leaders track key student performance indicators on a month-over-month basis, comparing performance to past semesters, and then they utilize the data to make real-time adjustments as needed.
Remediation and Student Support
Structured remediation is associated with improved readiness indicators. Meehan and Barker (2021) found that a prescribed remediation protocol helped high-risk students achieve the necessary Comprehensive Predictor scores associated with NCLEX success. House et al. (2021) also reported that a distance-delivered remediation course supported NCLEX-RN success among at-risk students during COVID-19 disruptions. These findings support Joyce’s use of individualized remediation plans, key concept reviews, ATI-guided remediation, and learning support integration.
Assessment Quality and Validity
NCLEX readiness decisions are only as strong as the assessments used to make them. Assessment validity requires alignment between course outcomes, program outcomes, licensure expectations, item design, administration conditions, and score interpretation. ATI’s technical manual emphasizes content validity, reliability, construct considerations, and standardized administration assumptions (Assessment Technologies Institute, 2020). Joyce’s assessment governance model, item piloting, psychometric review, and faculty item-writing development address these validity concerns at the program level.
Systems Thinking and Continuous Quality Improvement
A systems approach is necessary because NCLEX outcomes are influenced by multiple interacting variables.
NOTE:
- Curriculum alignment alone is insufficient if assessment quality is weak.
- Faculty development alone is insufficient if policies create inappropriate progression barriers.
- Remediation alone is insufficient if the risk is identified too late.
- Testing incentives alone are insufficient if students are not academically prepared.
The Joyce model addresses these interdependencies through feedback loops and shared accountability. The Feedback loops are outlined below:
| Data Source | Feeds Back To | Purpose |
| Assessment and exam analytics | Curriculum design and item revision | Prevent curriculum drift; improve assessment validity |
| NCLEX outcomes | The curriculum, policy review and readiness thresholds | Maintain defensibility and equity |
| Faculty performance data | Faculty development and support | Reduce instructional variability |
| Student success data | Intervention design and resource allocation | Focus efforts on high-impact strategies |
Outcome Metrics and KPI Tables
A comprehensive NCLEX readiness system requires clearly defined outcome measures, operational benchmarks, and continuous performance monitoring processes. Sustainable improvement in first-time NCLEX-RN pass rates cannot be achieved through isolated interventions or retrospective analysis alone. Rather, nursing programs must establish measurable indicators that evaluate readiness longitudinally across the educational continuum.
The following outcome metrics and key performance indicators (KPIs) were developed to support continuous quality improvement, early risk identification, regulatory accountability, and evidence-informed decision-making within the Joyce University NCLEX Readiness Model. These metrics intentionally combine leading indicators, such as predictor performance and CMS outcomes, with lagging indicators, such as first-time NCLEX-RN pass rates and time-to-test. This multidimensional approach reflects the understanding that NCLEX success is the product of interconnected academic, operational, instructional, and support systems rather than a single assessment event.
Importantly, these KPIs also support alignment with accreditation and regulatory expectations, including AACN Essentials competency development, CCNE outcomes assessment requirements, ACEN continuous improvement standards, and the Next Generation NCLEX emphasis on clinical judgment readiness. Collectively, these metrics allow institutions to monitor student progression, evaluate intervention effectiveness, identify curricular or assessment concerns, and ensure defensible readiness determinations through systematic and ongoing review processes. Refer to Table 1 below.
Table 1
Core NCLEX Readiness Outcome Metrics
| Outcome Area | Metric | Target or Threshold | Purpose |
| Licensure success | First-time NCLEX-RN pass rate | At or above national mean and at least 85% where applicable | Demonstrates graduate readiness and program effectiveness |
| Time-to-test | Percent testing within 45 days and 8 weeks | Increase each term | Reduces post-graduation decay and improves timely licensure |
| Readiness | ATI Comprehensive Predictor | At least 74% raw average across two attempts | Supports readiness determination and remediation planning |
| Readiness | VATI Greenlight | Required before ATT submission | Confirms individualized coaching and readiness completion |
| CMS performance | CMS Level 2 or higher | Increasing term-over-term | Monitors course-level mastery and content readiness |
| Course assessment | Exam failure rate per course | No greater than 20% beginning Summer 2026 | Identifies assessment, instruction, or curriculum concerns |
| Progression | Progression without repeat | At least 90% where feasible | Evaluates curriculum sequencing and support effectiveness |
| Re-entry success | Success of repeaters or re-entry students | At least 80% | Evaluates re-entry safety plans and remediation effectiveness |
Table 2, below, outlines the key leading, intermediate, operational, lagging, and quality indicators used to monitor and improve NCLEX-RN outcomes within a comprehensive readiness system. Together, these indicators provide a structured framework for continuous quality improvement by allowing institutions to identify risk early, evaluate intervention effectiveness, monitor operational efficiency, and assess long-term licensure outcomes. Leading indicators provide early warning signals that support proactive intervention, while lagging indicators evaluate the ultimate effectiveness of curriculum, instruction, assessment, and support systems. Operational and quality indicators further ensure that institutional processes, assessment validity, and program infrastructure remain aligned with student success and regulatory expectations. Collectively, these measures support evidence-informed decision-making, accountability, and sustainable NCLEX readiness improvement across the program.
Table 2
Leading and Lagging Indicators for NCLEX Improvement
| Indicator Type | Examples | Review Frequency | Responsible Area |
| Leading indicators | Course averages, CMS scores, predictor attempts, attendance, remediation completion | Weekly or biweekly | Faculty, student success, program leadership |
| Intermediate indicators | Course pass rates, progression rates, repeat course success, simulation/lab performance | End of course or term | Program leadership and curriculum/assessment committees |
| Operational indicators | Transcript processing time, ATT submission time, voucher utilization, testing date | Weekly during graduation/testing cycle | Registrar, advising, NCLEX readiness team |
| Lagging indicators | First-time NCLEX pass rate, all-taker pass rate, repeat pass rate, time-to-test outcomes | Monthly, quarterly, annually | Academic leadership and institutional effectiveness |
| Quality indicators | Item reliability, item discrimination, blueprint alignment, course variance reports | After each exam and term | Assessment committee and faculty |
The next table, Table 3, summarizes the major domains within the Joyce University NCLEX Readiness Model and translates each domain into actionable strategies that can be adopted by other nursing programs seeking to improve NCLEX-RN outcomes. The framework demonstrates that sustainable licensure success requires coordinated improvement across assessment systems, faculty development, student support, curriculum design, academic policies, and readiness infrastructure. By pairing institutional strategies with transferable program actions, the table provides a practical roadmap for implementing evidence-informed, systems-based approaches to NCLEX readiness and continuous quality improvement.
Table 3
Joyce Model Domains and Program-Level Improvement Actions
| Domain | Joyce Model Strategy | Transferable Program Action |
| Assessment | Centralized blueprinting, item review, item piloting, psychometric validation | Establish assessment governance and require post-exam item analysis |
| Faculty | Orientation, item-writing training, CBE preparation, mentoring, observation | Develop faculty readiness standards tied to NCLEX and clinical judgment outcomes |
| Readiness | Predictor benchmark, VATI Greenlight, dashboards, vouchers, fast transcripts | Use multiple readiness indicators and remove operational testing barriers |
| Policy | Review grading, progression, transfer, dismissal, and re-entry policies | Evaluate whether policies are valid, equitable, and outcome-aligned |
| Student support | At-risk dashboards, individualized remediation, re-entry plans | Intervene early using structured success plans and documented follow-up |
| Curriculum | NCLEX and AACN mapping, ATI overlay, sequencing, integrated modalities | Conduct annual curriculum mapping and variance review |
Accreditation and Regulatory Implications
CCNE Implications
All Joyce University Bachelor’s degree nursing programs are accredited by the Commission on Collegiate Nursing Education (CCNE). The CCNE 2024 Standards require programs to demonstrate achievement of required program outcomes related to licensure. Programs may demonstrate licensure pass-rate achievement through several approaches, including first-time pass rates of 80% or higher for each campus/site and track for the most recent calendar year, all-taker pass rates of 80% or higher, or three-year aggregated approaches (Commission on Collegiate Nursing Education [CCNE], 2024). CCNE also expects programs to provide aggregate student outcome data, including completion rates, licensure pass rates by campus/site and track, certification pass rates where applicable, employment rates, and evidence that data are analyzed and used for ongoing program improvement (CCNE, 2024).
The Joyce model aligns strongly with these expectations because it does not treat NCLEX performance as an isolated annual statistic. Instead, it creates a continuous improvement system in which NCLEX outcomes, assessment analytics, faculty performance, and student success data inform curriculum, policy, and intervention decisions.
ACEN Implications
Our associate’s degree nursing program is accredited by the Accreditation Commission for Education in Nursing (ACEN). ACEN Standard 5 focuses on outcomes and requires nursing programs to demonstrate student learning and program outcome achievement. Although specific benchmarks and reporting structures vary by program type and accreditation context, the underlying expectation is that programs systematically evaluate outcomes, analyze data, and use findings for program improvement. For programs with declining NCLEX outcomes, an integrated model such as Joyce’s provides a stronger accreditation response than a narrow remediation plan because it demonstrates root-cause analysis, shared accountability, data-informed decision-making, and sustained monitoring.
The Joyce model is especially useful from an ACEN lens because it connects NCLEX outcomes to curriculum, faculty, students, policies, and assessment quality. This creates a defensible narrative that the program is not merely reacting to pass-rate concerns but has implemented a structured, measurable, and continuously monitored improvement system.
Board of Nursing and Public Protection Implications
Boards of nursing are concerned not only with pass rates but also with public protection and the readiness of graduates to enter practice safely. A model that strengthens assessment validity, clinical judgment development, remediation, and timely testing supports the public protection function of nursing regulation. The NGN emphasis on clinical judgment further reinforces the need for programs to align learning activities, simulation, clinical experiences, and assessments with entry-level decision-making demands.
Recommendations for Nursing Programs Seeking to Improve NCLEX-RN Outcomes
1. Conduct a Full-System Diagnostic Review
Programs should begin by examining the entire readiness ecosystem rather than assuming the problem is limited to students or a single course. The review should include admissions data, progression data, course outcomes, standardized assessment performance, faculty preparation, curriculum mapping, exam quality, remediation effectiveness, and time-to-test patterns.
2. Build a Multi-Indicator Readiness Model
Programs should avoid overreliance on a single predictor, exit exam, or course grade. A stronger readiness model includes course performance, CMS or specialty assessment performance, comprehensive predictor results, remediation completion, clinical judgment performance, faculty input, and student engagement data.
3. Establish Assessment Governance
Programs should implement standardized blueprinting, item-writing training, item review, exam analysis, and psychometric review. Assessment quality should be monitored as a program-level quality indicator rather than left solely to individual faculty preference.
4. Align Curriculum to NGN Clinical Judgment Expectations
Programs should map curriculum to the NCLEX test plan, NCJMM cognitive operations, AACN Essentials competencies, and program outcomes. Clinical judgment should be developed progressively through didactic learning, unfolding case studies, simulation, lab, clinical, and debriefing.
5. Implement Early Alert Dashboards
Programs should identify risk before course failure or graduation. Dashboards should include academic performance, standardized assessment scores, attendance, progression history, remediation completion, and engagement with support services.
6. Standardize Remediation
Remediation should be structured, individualized, documented, and connected to missed content and clinical judgment deficits. Students should receive clear expectations, targeted resources, faculty follow-up, and accountability checkpoints.
7. Strengthen Faculty Capability
Faculty development should include NCLEX test plan updates, NGN item-writing, clinical judgment pedagogy, exam analysis, remediation coaching, and competency-based education principles. Faculty data should be used to guide support, not merely evaluation.
8. Review Policies for Validity and Equity
Programs should evaluate whether grading, progression, dismissal, transfer credit, re-entry, and standardized testing policies are evidence-informed and consistently implemented. Policies should protect academic standards while avoiding unnecessary barriers that are not predictive of licensure success.
9. Reduce Time-to-Test
Programs should examine operational delays between graduation and NCLEX testing. Transcript processing, ATT support, testing fee barriers, advising, and scheduling assistance should be reviewed and improved.
10. Create a Continuous Improvement Rhythm
NCLEX performance should be reviewed continuously through formal governance structures. Programs should establish monthly and quarterly NCLEX readiness reviews, annual curriculum variance reviews, post-exam assessment reviews, and regular reporting to academic leadership. Annual program reviews are not enough.
Discussion
The Joyce University model demonstrates that NCLEX improvement is most defensible when it is framed as academic quality improvement rather than test preparation alone. This distinction matters. Programs that focus only on test preparation may improve short-term performance while leaving deeper curricular, assessment, and faculty issues unresolved. In contrast, programs that build integrated readiness ecosystems can improve NCLEX outcomes while strengthening overall educational quality.
The model also supports equity. Overreliance on a single high-stakes gate can disproportionately harm students when the gate is not sufficiently valid, when remediation is inconsistent, or when operational barriers delay testing. A multi-indicator model allows programs to maintain rigor while ensuring that readiness decisions are based on a fuller body of evidence.
Finally, the model supports accreditation defensibility. Accreditors expect programs to analyze outcomes, identify variances, implement improvements, and evaluate effectiveness. The Joyce ecosystem provides a structure for demonstrating that NCLEX outcomes are actively managed through a formal quality system.
Conclusion
NCLEX-RN outcomes are not isolated student outcomes; they are institutional outcomes produced by curriculum, assessment, faculty, policy, student support, and operational systems. Joyce University’s Comprehensive NCLEX Readiness Model offers a practical and evidence-informed example of how nursing programs can improve first-time pass rates through intentional design, predictive analytics, early intervention, assessment governance, faculty development, policy alignment, and continuous feedback loops.
We have had early, clear, and measurable NCLEX_RN pass rate success with initial implementation. We will continue to test and refine this model over the next two years. Programs seeking to improve NCLEX-RN outcomes should move beyond reactive remediation and adopt integrated readiness ecosystems that work for their unique system and student demographics. Such systems are better aligned with the Next Generation NCLEX, competency-based education, accreditation expectations, and the public protection mission of nursing education.
References
American Association of Colleges of Nursing. (2021). The Essentials: Core competencies for professional nursing education. Author.
Assessment Technologies Institute. (2020). Technical manual for the RN Comprehensive Predictor 2019. Assessment Technologies Institute.
Breckenridge, D. M., Wolf, Z. R., & Roszkowski, M. J. (2012). Risk assessment profile and strategies for success instrument: Determining prelicensure nursing students’ risk for academic success. Journal of Nursing Education, 51(3), 160–166. https://doi.org/10.3928/01484834-20120113-03
Commission on Collegiate Nursing Education. (2024). Standards for accreditation of baccalaureate and graduate nursing programs. American Association of Colleges of Nursing.
Cummings, J. A. F., Kennard, D., Egan, J., Aryal, S., & McVey, C. (2024). An exploratory study: Indicators of NCLEX-RN success. Teaching and Learning in Nursing. https://doi.org/10.1016/j.teln.2024.07.004
Giddens, J. F. (2022). The revised AACN Essentials: Implications for nursing regulation. Journal of Nursing Regulation, 13(1), 53–56. https://doi.org/10.1016/S2155-8256(22)00009-6
House, S. K., Hubbard, J., & Bacus, R. (2021). Adapting NCLEX-RN remediation during the COVID-19 pandemic. Teaching and Learning in Nursing, 17(1), 74–78. https://doi.org/10.1016/j.teln.2021.09.006
Lewis, L. S., Willard, V., & Staudt, C. (2023). Effect of a commercial NCLEX-RN preparation product on first-time pass rates. Nursing Reports, 13(3), 1141–1150. https://doi.org/10.3390/nursrep13030098
Meehan, C. D., & Barker, N. (2021). Remediation for NCLEX-RN success in high-risk nursing students. Teaching and Learning in Nursing, 16(3), 254–257. https://doi.org/10.1016/j.teln.2021.01.005
National Council of State Boards of Nursing. (2023a). Next Generation NCLEX. https://www.nclex.com/next-generation-nclex.page
National Council of State Boards of Nursing. (2023b). Clinical Judgment Measurement Model. https://www.nclex.com/clinical-judgment-measurement-model.page
National Council of State Boards of Nursing. (2026). NCLEX pass rates. https://www.ncsbn.org/exams/exam-statistics-and-publications/nclex-pass-rates.page
Appendix A

{kind=link}
Related Articles

March 19
How to Reduce Stress and Anxiety When Preparing for the NCLEX
As one of the most pivotal academic challenges any aspiring nurse will face, the National Council Licensure Examination- Registered Nurse...
March 19
After completing your clinical rotations, courses, and graduating from nursing school, there is one final test to pass before becoming...

November 01
After you've earned your ASN degree or 3-year BSN degree, registering for the NCLEX is a crucial step towards obtaining...
October 26
How to Break Down NCLEX Questions
The NCLEX is different from most tests you’ve taken during school. Instead of measuring your basic nursing knowledge, the NCLEX...
May 05
Becoming a nurse means passing the National Council Licensure Examination, better known as the NCLEX. The test, proctored by the...